
I recently spoke with a woman whose story has stayed with me.
Her brother died from a heart attack in his 40s.
The shocking part?
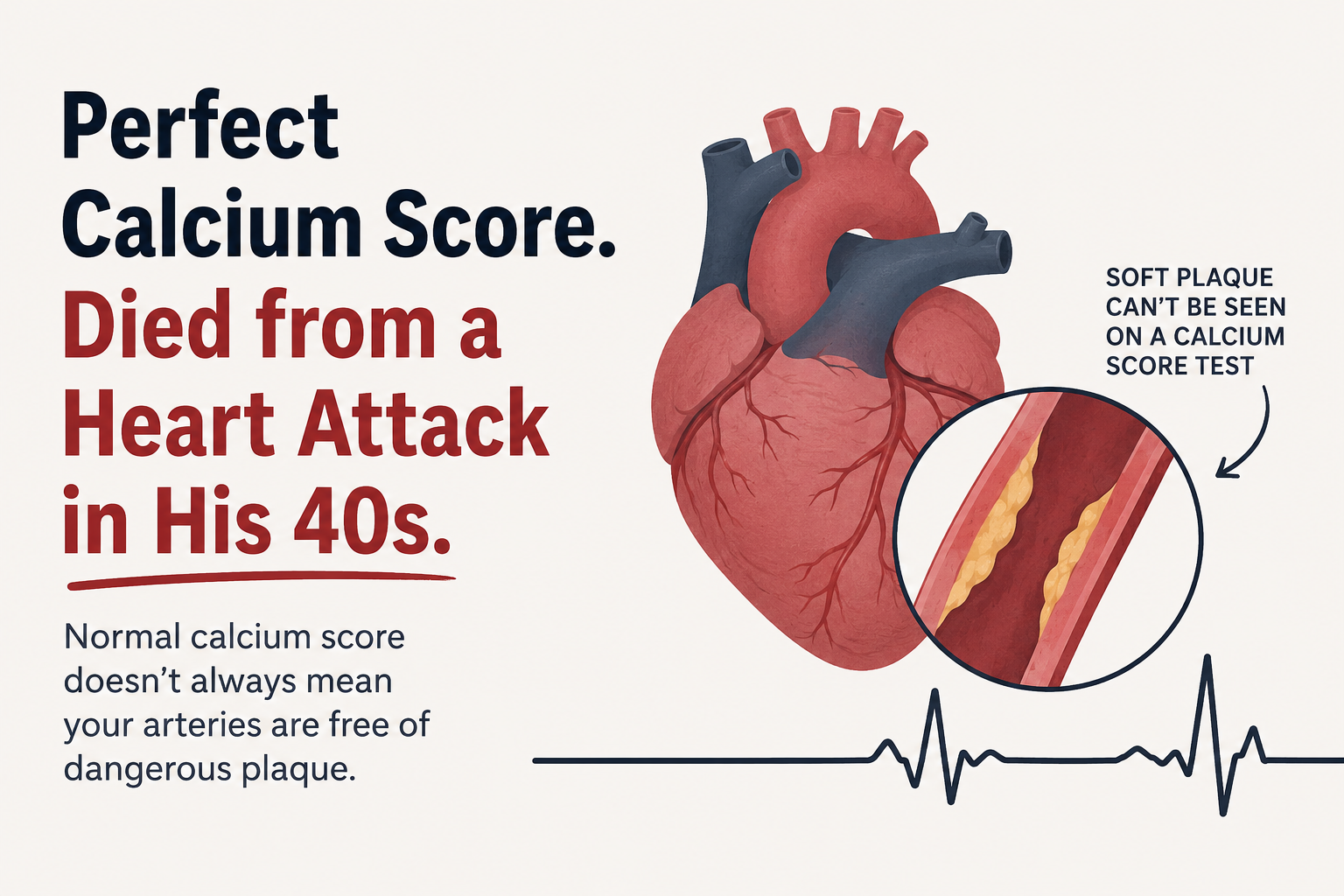
He had been told his coronary calcium score was perfect.
Most people believe a calcium score of zero means they have nothing to worry about. While a calcium score is an excellent test for detecting calcified plaque, it does not detect all plaque.
Some plaque is soft (non-calcified). This type of plaque can grow silently, become unstable, rupture, and trigger a heart attack—even when a calcium score is zero.
After his death, additional testing showed he had approximately 90% blockage in his left anterior descending (LAD or "widow maker") artery, largely from soft plaque.
He also had hereditary hemochromatosis, an iron overload disorder that had not been properly managed.
Why does this matter?
Excess iron doesn't just accumulate in the liver.
It can increase oxidative stress, damage blood vessels, and contribute to inflammation throughout the body. Research suggests these processes may play a role in the development and progression of cardiovascular disease.
For many people with hereditary hemochromatosis, proper diagnosis and treatment can dramatically reduce iron levels and may help lower long-term health risks.
Does this mean everyone needs more testing?
A coronary calcium score remains a valuable screening tool for many patients.
However, it is important to understand what the test can and cannot tell you.
For individuals with a strong family history of premature heart disease, hereditary hemochromatosis, elevated genetic risk, persistent symptoms, or other significant risk factors, your physician may determine that additional testing—such as a coronary CT angiogram (CCTA)—is appropriate. New AI-assisted analysis platforms, including Cleerly, can help physicians evaluate both calcified and soft plaque on these scans.
The bottom line
A "normal" test result is not always the whole story.
Understanding your genetics, iron status, family history, and overall cardiovascular risk provides a much more complete picture of your health.
If you or someone you love has hereditary hemochromatosis, unexplained high ferritin, elevated transferrin saturation, or a strong family history of heart disease, don't ignore it.
Knowledge today can prevent tragedy tomorrow.
If you'd like to learn more about how iron overload affects the body—including the heart, brain, liver, hormones, and joints—I invite you to read my book, The Iron Curse, or attend one of my educational workshops on hereditary hemochromatosis.
Because sometimes the biggest risk isn't what a test finds—it's what the test can't see.
To your health,
Dr. Christy Sutton
Register for Dr. Sutton's Heart Health Labrogenomics Workshop.
Could Resveratrol Help Protect the Heart and Brain in Hereditary Hemochromatosis?
Hereditary hemochromatosis causes the body to absorb too much iron, and excess iron can generate harmful free radicals through oxidative stress. Over time, this oxidative damage may contribute to injury in the heart, blood vessels, and brain. Resveratrol, a natural polyphenol found in grapes, berries, and Japanese knotweed, has been extensively studied for its antioxidant and anti-inflammatory properties. Laboratory and animal studies suggest that resveratrol may help reduce iron-induced oxidative stress, support healthy mitochondrial function, protect the cells lining blood vessels, and reduce inflammation that contributes to cardiovascular and neurological damage. It has also been shown to activate protective pathways, including SIRT1, which are involved in healthy aging and cellular repair. While resveratrol is not a treatment for hereditary hemochromatosis and should never replace therapeutic phlebotomy or other physician-directed care, emerging research suggests it may serve as a supportive strategy for protecting the heart and brain from some of the oxidative damage associated with iron overload. More human clinical trials are needed to determine the optimal dose and its long-term benefits in people with hereditary hemochromatosis.
